Fill Your Cna Shower Sheets Form
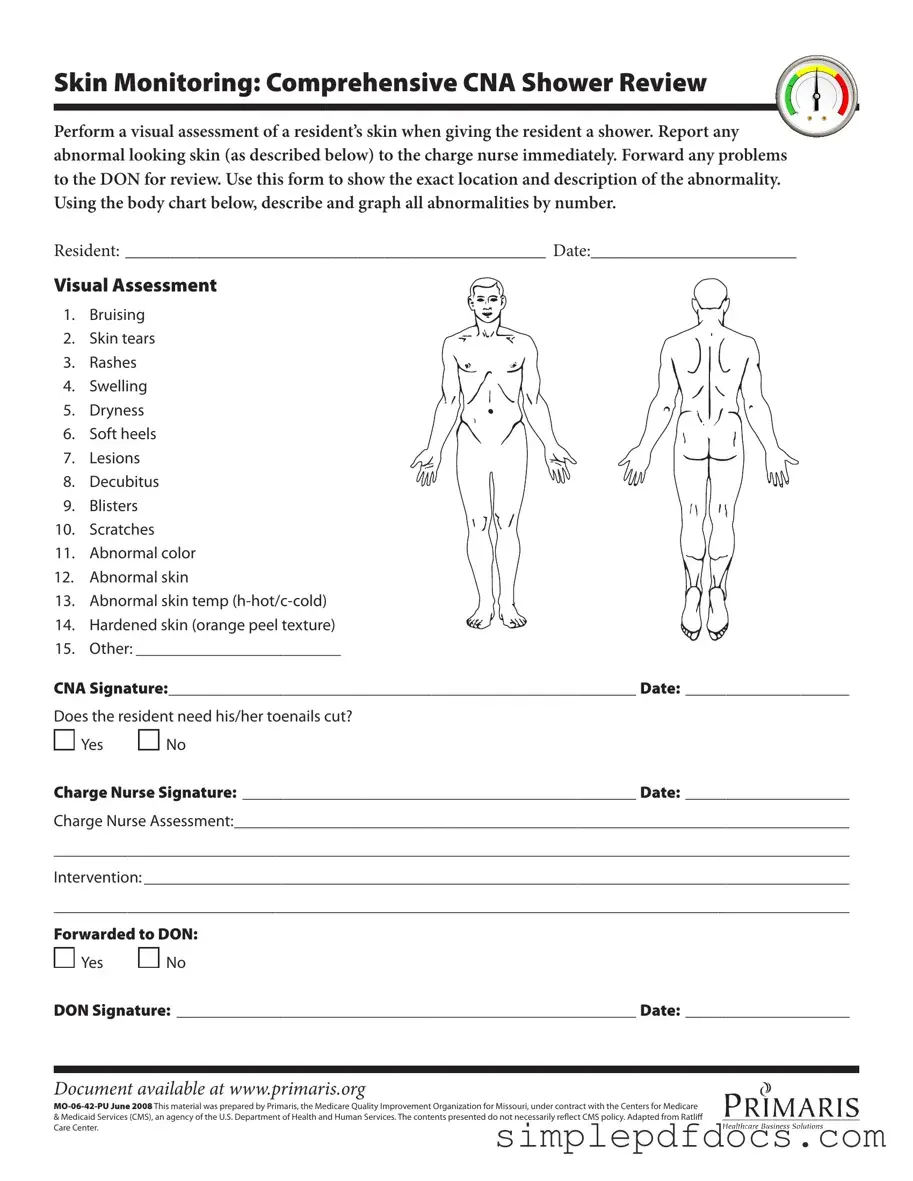
The CNA Shower Sheets form is an essential tool for certified nursing assistants (CNAs) to ensure thorough skin monitoring during resident showers. This form facilitates a detailed visual assessment of a resident's skin, allowing CNAs to identify and document any abnormalities, such as bruising, skin tears, rashes, and more. Each identified issue must be reported to the charge nurse immediately, ensuring that proper care is provided without delay. The form includes a body chart for CNAs to accurately mark the location of each abnormality, enhancing clarity in communication. Additionally, it prompts CNAs to assess the condition of the resident's toenails, determining if a trim is necessary. The charge nurse then reviews the findings and can make further assessments or interventions as needed. Lastly, the form requires the charge nurse's and Director of Nursing's (DON) signatures to confirm that the information has been reviewed and any necessary actions have been taken. This structured approach not only promotes resident safety but also ensures compliance with healthcare standards.
More PDF Templates
Free Doctors Note - This form is crucial for ensuring that students and employees are treated fairly regarding attendance policies.
Form 10-2850c - The VA uses the information gathered from the 10-2850c form to ensure compliance with federal hiring regulations.
A Hold Harmless Agreement form is essential for individuals and businesses in Texas to outline the responsibilities and liabilities involved in various transactions. By understanding this legal document, parties can ensure that they are protected from unforeseen risks and losses. For those interested in securing their financial and legal safety, visiting texasformspdf.com/ can provide a streamlined process to fill out the Texas Hold Harmless Agreement form with ease.
W9 Form 2022 - The W-9 form plays a vital role in the gig economy, ensuring compliance.
Document Specifics
| Fact Name | Description |
|---|---|
| Purpose | The CNA Shower Sheets form is used to document skin assessments during resident showers. |
| Visual Assessment | CNA staff perform a visual assessment of the resident’s skin and report any abnormalities. |
| Abnormalities | Common skin issues to look for include bruising, skin tears, rashes, and swelling. |
| Documentation | Details about skin abnormalities are recorded, including location and description on the form. |
| Forwarding Issues | Any identified problems must be reported to the charge nurse and forwarded to the Director of Nursing (DON). |
| Signature Requirement | The form requires signatures from both the CNA and the charge nurse to ensure accountability. |
| Toenail Care | The form includes a section to indicate if the resident needs toenail trimming, enhancing overall care. |
| Body Chart | A body chart is provided for CNAs to graphically indicate the location of any skin abnormalities. |
| Legal Compliance | This form is governed by state-specific regulations and should be used in accordance with local laws. |
| Availability | The form can be accessed online at www.primaris.org, ensuring easy availability for healthcare providers. |
How to Write Cna Shower Sheets
Filling out the CNA Shower Sheets form is an important task that requires attention to detail. This form helps ensure that any abnormalities in a resident's skin are documented and communicated effectively. Follow these steps to complete the form accurately.
- Fill in the resident's name: Write the full name of the resident at the top of the form where it says "RESIDENT."
- Enter the date: Write the current date next to the "DATE" section.
- Conduct a visual assessment: As you give the resident a shower, carefully examine their skin for any abnormalities.
- Document abnormalities: For each abnormality you observe, refer to the list provided (e.g., bruising, skin tears, rashes). Use the body chart to indicate the exact location of each issue by numbering them.
- Describe each abnormality: Next to each number, provide a brief description of the observed condition.
- Check if toenails need cutting: Indicate whether the resident needs their toenails cut by circling "Yes" or "No."
- Sign the form: At the bottom, sign your name where it says "CNA Signature" and include the date.
- Charge nurse signature: After completing the form, present it to the charge nurse for their signature and date.
- Charge nurse assessment: The charge nurse should document their assessment in the space provided on the form.
- Forward to the DON: Indicate whether the form has been forwarded to the Director of Nursing (DON) by circling "Yes" or "No." If applicable, obtain the DON's signature and date.
Dos and Don'ts
When filling out the CNA Shower Sheets form, there are important guidelines to follow. Here are eight things to do and not do:
- Do perform a thorough visual assessment of the resident's skin during the shower.
- Do report any abnormal skin findings to the charge nurse immediately.
- Do accurately describe and graph all abnormalities using the body chart provided.
- Do ensure that the resident's name and date are clearly filled out at the top of the form.
- Don't ignore any signs of abnormality, such as bruising or skin tears.
- Don't leave the form incomplete; all sections must be filled out properly.
- Don't forget to sign the form with your CNA signature and date it.
- Don't delay forwarding any concerns to the Director of Nursing (DON) for further review.
Documents used along the form
When working with the CNA Shower Sheets form, several other documents and forms may be necessary to ensure comprehensive care and accurate record-keeping. Each of these documents serves a specific purpose in the care process, enhancing communication among healthcare providers and ensuring that residents receive the best possible attention.
- Incident Report: This document is used to record any unusual events or accidents that occur during a resident's care. It includes details about what happened, who was involved, and any immediate actions taken. This report helps identify patterns that may need addressing to improve safety.
- Skin Assessment Form: This form provides a detailed evaluation of a resident’s skin condition over time. It includes sections for documenting the location, size, and type of any skin issues. Regular assessments can help track changes and ensure timely interventions.
- Care Plan: A care plan outlines the specific needs and goals for each resident based on their individual health conditions. It includes interventions, responsibilities, and timelines for achieving desired outcomes. This document is essential for coordinating care among different staff members.
- Notice to Quit Form: This legal document is essential for landlords to formally notify tenants of lease violations or non-renewal of tenancy, giving them a chance to address issues before further legal action is taken. More information can be found at https://floridaforms.net/blank-notice-to-quit-form.
- Nursing Notes: These notes are used by nursing staff to document observations, assessments, and any changes in a resident's condition. They provide a continuous record that can be referenced by other caregivers, ensuring that everyone is informed about the resident's status.
- Medication Administration Record (MAR): This record tracks all medications administered to a resident, including dosages and times. It is crucial for preventing medication errors and ensuring that residents receive their prescribed treatments consistently.
Utilizing these documents in conjunction with the CNA Shower Sheets form creates a more thorough and organized approach to resident care. Each form plays a vital role in maintaining high standards of health and safety, fostering a collaborative environment among healthcare providers.